
How many of you out there have experienced vertigo? How many times have you simply rolled over in bed or stood up and felt dizzy? Are you one of those people who says you "just got up too quickly"?! Maybe you should get assessed for vertigo by a physiotherapist trained in vestibular rehabilitation. Physiotherapy can offer immediate resolution of your vertigo symptoms without the need for tablets or bed rest. Let us explain how!
What is Vertigo?
Vertigo is actually a symptom, and not a diagnosis. That means that when you're told you have vertigo, that's really only half the story. Vertigo is that horrible sensation where the world is spinning. It's an incredibly debilitating sensation as you struggle to walk, drive or even stand. Therefore you yourself can identify when you have vertigo, the tricky part is figuring out which type of vertigo it is.
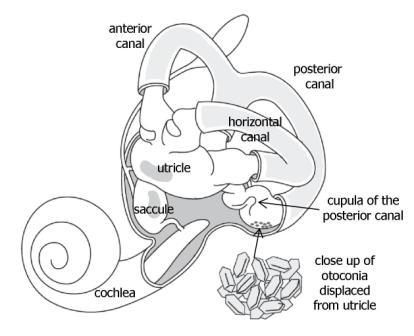
Benign Paroxysmal Positional Vertigo or BPPV is the most common cause of vertigo. This is when tiny crystals (called otoconia) get displaced from the utricle (see diagram below) and can become either free-floating in the canals or at the end of each canal in your inner ear. Each canal has a specific test to determine whether the otoconia are located in it and from there your treatment plan can be decided.
Benign Paroxysmal Positional Vertigo or BPPV is the most common cause of vertigo. This is when tiny crystals (called otoconia) get displaced from the utricle (see diagram below) and can become either free-floating in the canals or at the end of each canal in your inner ear. Each canal has a specific test to determine whether the otoconia are located in it and from there your treatment plan can be decided.
Treatment
The most commonly affected canal is the posterior canal and to test this the Hallpike Dix Test is performed. If positive, the eyes will move in a certain direction and the vertigo symptoms will be reproduced. From that position we can go straight into treatment which involves moving the head in certain directions to move the otoconia out of the canal and back into the utricle. This manoeuvre can be done a few times in one treatment but generally it resolves symptoms immediately. It's important you don't lie down for a couple of hours afterwards as this could undo all of the good work and allow those otoconia to get back into the canal!
The most commonly affected canal is the posterior canal and to test this the Hallpike Dix Test is performed. If positive, the eyes will move in a certain direction and the vertigo symptoms will be reproduced. From that position we can go straight into treatment which involves moving the head in certain directions to move the otoconia out of the canal and back into the utricle. This manoeuvre can be done a few times in one treatment but generally it resolves symptoms immediately. It's important you don't lie down for a couple of hours afterwards as this could undo all of the good work and allow those otoconia to get back into the canal!
Research
A recent Cochrane review by Hilton & Pinder (2014) found that these re-positioning manoeuvres (as described above) are effective in completely resolving your vertigo in 56% of cases. There is unfortunately a recurrence rate of 36% which is why McDonnell & Hillier (2015) recommend a combination of vestibular rehabilitation and these manoeuvres to keep your vertigo at bay. Research in vestibular rehabilitation is certainly a growing area and there are currently several studies being carried on other forms of re-positioning manoeuvres.
A recent Cochrane review by Hilton & Pinder (2014) found that these re-positioning manoeuvres (as described above) are effective in completely resolving your vertigo in 56% of cases. There is unfortunately a recurrence rate of 36% which is why McDonnell & Hillier (2015) recommend a combination of vestibular rehabilitation and these manoeuvres to keep your vertigo at bay. Research in vestibular rehabilitation is certainly a growing area and there are currently several studies being carried on other forms of re-positioning manoeuvres.
One thing is for sure, vestibular rehabilitation is definitely worth a try for those of you experiencing vertigo or dizziness symptoms! You can contact us here at PhysioElite for an assessment any time or if you've any questions!
References
- http://vestibular.org/understanding-vestibular-disorders/types-vestibular-disorders/benign-paroxysmal-positional-vertigo (Accessed on 21/11/2016)
- Hilton MP, Pinder DK. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database of Systematic Reviews 2014, Issue 12. Art. No.: CD003162. DOI: 10.1002/14651858.CD003162.pub3.
- Hunt WT, Zimmermann EF, Hilton MP. Modifications of the Epley (canalith repositioning) manoeuvre for posterior canal benign paroxysmal positional vertigo (BPPV). Cochrane Database of Systematic Reviews 2012, Issue 4. Art. No.: CD008675. DOI: 10.1002/14651858.CD008675.pub2.
- McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database of Systematic Reviews 2015, Issue 1. Art. No.: CD005397. DOI: 10.1002/14651858.CD005397.pub4.
 RSS Feed
RSS Feed
